
The low prevalence of infections make Test and Trace expensive, time consuming and almost meaningless.
The Basic Arithmetic
As usual, I am writing about the SARS-CoV2 (SC2) numbers from a Scottish perspective but the general conclusions apply to any country.
It is quite apparent from pronouncements from the First Minister, Ms Sturgeon, that she has no idea what the numbers she is communicating to the general public actually mean.
The Daily Record journalists Chris McCall and Peter Davidson wrote the following nonsense: “Over the last 24 hours 47 new cases of the deadly virus were identified with no deaths since July 16.”
It is perhaps the noted failings of the Scottish education system (once regarded as one of the finest in the world) that a journalist could write such condescending drivel.
A deadly virus has not killed anyone in a month?
The 47 cases increased to 65 following Sturgeon’s usual cringe-worthy daily speech on the 14th August.
Tara Fitzpatrick of the same rag tells us that“The total number of cases of the virus now stands at 19,238 throughout the country.”
The first major problem is that there was 13,991 ‘tests’ given to identify these 65 ‘cases’. That’s a 0.46% rate of detection.
The second major problem is that there cannot possibly be 19,238 cases throughout the country.
Quite apart from the fact that nearly 5,000 of them have died (with COVID19 mentioned on the Death Certificate), the figure is a cumulative number of those who have tested ‘positive’ for SC2.
So when does a ‘COVID19 case’ cease to be a ‘case’?
The estimated time from infection to either death or release from hospital is 22-24 days. Anyone who tested ‘positive’ more than 24 days before today cannot be considered a case. They have either recovered or are now dead.
Let’s be kind and measure the Government figures from July 1st 2020. They are as I expected, a complete mess. Before 1st April (17,007 tests) we don’t know where they were taken. The total test numbers do not agree with each other. They are all over the place. A note excusing the mess reads:
As of 8 July, (iv) includes numbers of home tests and other tests through the social care portal that were not previously available from the UK Government (UKG) testing programme.
The increase in the cumulative figures in (iv) on 8 July is due to the addition of the backlog of care home portal tests and home tests to the database. It is not possible to incorporate these in the previous daily figures.
However, we have some numbers we can work with from 1st July
- 987 people have tested positive.
- There have been 435,617 tests. (179,933 through NHS labs, 261,684 through UK Gov Tests)
The number tested is, without doubt, a biased sample. We don’t know who was tested, where or by whom. But it amounts to 8% of the total 5.5 million population of Scotland.
The worst case scenario is that 987 people in the country may have been infected by SC2.
That is 0.22% of people tested have shown as ‘positive’. This is the prevalence of SC2 in Scotland.
This is the number that Sturgeon relies on to continue the “war against the virus”.
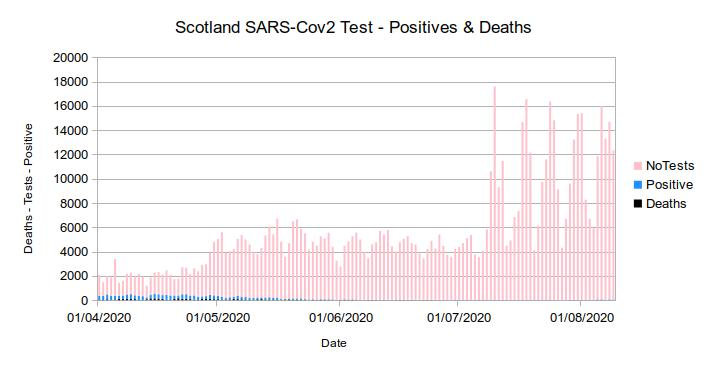
The graph above shows the true extent of SC2 in Scotland. I prefer to show a graph from actual data to scale to give a realistic picture of what is actually happening.
You will need a magnifying glass to see the number of deaths per day and the number of ‘positive’ test results per day. That’s not an illusion. It is the actual numbers.
Feel free to disagree, but the numbers strongly suggest that SC2 had burned out by mid May. Positive test results have been almost non-existent since then despite the massive increase in testing.
Before we get on to the mathematics of SC2 testing, I would like to look at the overall cost of this search for the proverbial needle in a haystack.
Now I don’t know the actual cost of a single test the Scottish government actually pays. I did look at the Lloyds pharmacy website and the cost of 1 antibody kit is £59 and a Swab Test Kit is £99. I know that the government will have extra overheads including labour, lab costs, transportation, handling etc. So let’s say a range from £90 to £150 per test.
Given 435,617 tests from 1st July we have guesstimates of:
- £34.85 million to £65.34 million spent so far to find nothing.
The Mathematics
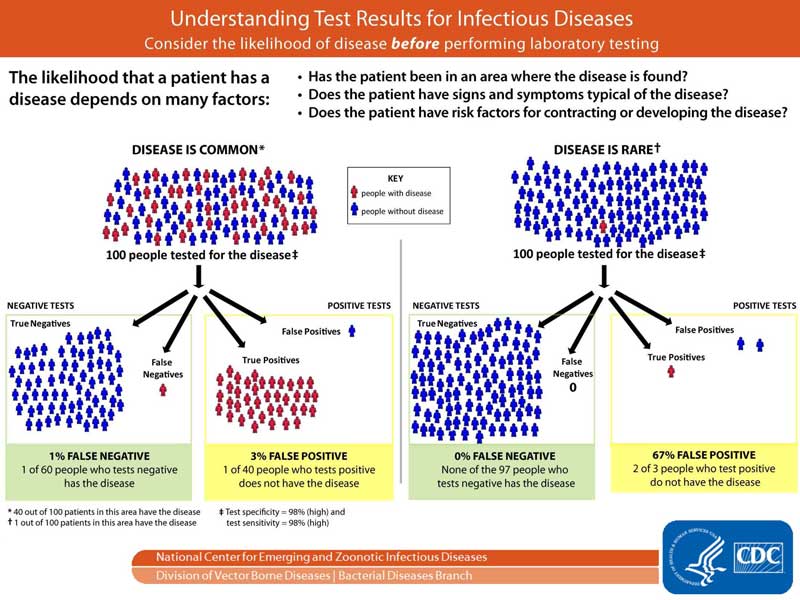
What we want to know is the probability of being infected with SC2 given that you test positive.
You may think that a PCR test which is 97% accurate means that it is 97% certain that you have been infected. This would seem like a reasonable assumption given the accuracy of the test.
In this example I will use Bayes Theorem to calculate the likelihood of being positive given that you test positive. Things are not quite as simple as they seem.
Bayes can be described in its simplest terms as: “a mathematical equation used in probability and statistics to calculate conditional probability. In other words, it is used to calculate the probability of an event based on its association with another event.”
As an example. Let’s say Liverpool FC are playing Norwich at Anfield. Your initial estimate based on prior games, league position and player strength may lead you to the conclusion that the chance of a Liverpool win would be 80%. Then you learn that 3 Liverpool players have been sent off in the first 20 minutes. Liverpool’s chance of a win now drops to 10%.
Your prior beliefs change when new information ids known.
Given that a SC2 test is 97% accurate what is the likelihood that you are really positive given that there is only a 0.3 chance of having the disease. We start with the assumption that the test is 97% accurate and then update our assumption with the 0.3% prevalence.
At it’s simplest, Bayes Theorem can be written as :
Where P(A|B) means the probability (P) of event A given event B.
Before we start, it is important to describe a few of the terms we will use.
Sensitivity
This the probability expressed as a static number of testing positive and actually being positive.
Some tests will be classified as having 99% specificity but it is important to know that this is not a static number. It can vary tremendously on different factors. For this analysis 97% is used.
Specificity
This is the probability expressed as a static number of testing negative and actually being negative. Again, this can vary tremendously. For this analysis 97% is used.
Prevalence
This is the probability expressed as a static number of the amount of people actually being infected in the population. 0.3% has been used in this analysis.
No Covid
This is the people who do are not infected. 1 – prevalence. 99.7% has been used in this analysis based on the positive test returns.
False Positive
This is the probability of testing positive without being infected. 3% has been used in this analysis. 1 – sensitivity.
False negative
This is the probability of testing negative and being infected. 3% has been used in this analysis. 1 – specificity.
When working out the equations, all percentage figures are written as 97% = 0.97 etc.
Writing this out in terms of Bayes we come up with the following formula:

P(Pos | Cov) is Sensitivity = 0.97
P(Cov) is Prevalence = 0.003
P(Pos|NoCov = 0.03
P(NoCov) = 0.997
Gives 0.97 * 0.003 = 0.00291
Divided by:
0.00291 + (0.03 * 0.997) = 0.00291 + 0.02991 = 0.03282
Gives 0.00291 / 0.03282 = 0.08872
Or an 8.87% chance of actually having the disease.
Conclusion
Not only has it been shown that the number of cases has been wildly misreported and the prevalence of the SC2 virus has almost disappeared, the outbreak almost certainly burned itself out in mid May.
Using Bayes analysis and conditional probability shows that the likelihood of being infected with SC2, even if you test positive is around 10%. (Probabilities are not static numbers. They will have a range given the observed data)
Despite media reports of SC2 infections being underestimated, the opposite is true. They are grossly overestimated.
One further point which I think is vital is that people, whether asymptomatic or symptomatic, are not being tested for anything other that SC2.
There is a large amount of time, money and effort being spent trying to find something which has such a low probability of actually being measured.
I’m not a virologist or an epidemiologist or a serologist. I just look at the numbers.
Notes
- Thanks to Michael A Lewis for the graphic of Bayes formula as related to SC2. This is a must read article from the Significance magazine published by the Royal Statistical Society and the American Statistical Association.
- In medicine the use of Bayes Theorem is called PPV (Positive Predictive Value). There are many online calculators available to check the numbers for yourself.
- The sensitivity and Specificity figures used in the calculations do NOT reflect reality. They are used for example purposes only.


I was looking through some of your articles on this internet site and I believe this website is real instructive! Keep on putting up.
LikeLike